Dr Karin Weyer, MD, Coordinator, Laboratories, Diagnostics and Drug Resistance; Dr Dennis Falzon, MD, Medical Officer; Dr Ernesto Jaramillo, MD, Phd, TeamLeader, Drug-resistant TB policies; Dr Matteo Zignol, MD, Team Lead, Global Project on Anti-tuberculosis Drug Resistance Surveillance; Fuad Mirzayev and Professor Mario Raviglione, MD, Director, Global TB Programme, World Health Organization, Geneva, Switzerland
Tuberculosis (TB) strains with rifampicin or multidrug resistance (defined as, at least, combined rifampicin and isoniazid resistance) – MDR/RR-TB – require more complex, costly management than drug-susceptible TB. The global response to MDR/RR-TB will determine if the targets set in the context of the new End TB Strategy of the World Health Organization (WHO) are achieved. In 2015, WHO estimated that 580,000 incident MDR/RR-TB cases and 250,000 MDR/RR-TB deaths occurred globally. However, country reports to WHO show that only 30% of TB patients notified worldwide are tested for MDR/RR-TB, 22% of those eligible start MDR-TB treatment and just over one half of them complete treatment successfully. Strong political commitment and increased funding for research and universal diagnosis and effective treatment for MDR/RR-TB are direly needed.
Antimicrobial resistance (AMR) has become one of the dominating, and most pressing, global concerns in public health (1). Yet a silent epidemic at the core of AMR often goes largely unnoticed and neglected – tuberculosis (TB), the world’s number one infectious disease killer (2). Multidrug-resistant TB (MDR-TB, defined as resistance to, at least, rifampicin and isoniazid) and rifampicin-resistant TB (RR-TB) are especially devastating.
Patients with MDR-TB and RR-TB (MDR/RR-TB) require radical changes in treatment compared to those with drug-susceptible TB. They need prolonged treatment (often up to two years) with costly, highly toxic and much less effective second-line medicines, of which there is only a limited number. Moreover, once fluoroquinolones and injectable agents – leading components in second-line treatment regimens – are compromised by additional drug resistance (extensively drug-resistant TB, XDR-TB, defined as MDR-TB plus additional resistance to at least the two most important groups of second-line medicines: the fluoroquinolones and the injectable agents kanamycin, amikacin and capreomycin), treatment becomes extremely difficult.
Patients with drug-resistant TB face agonising, prolonged suffering and often permanent disability while on second-line treatment, together with devastating economic hardship, stigma and discrimination. On top of the clinical toll taken by M/XDR-TB treatment, patients often face catastrophic economic repercussions, pushing them into extreme poverty. Once treatment options are exhausted, patients and health services are confronted by numerous ethical, legal and human rights challenges, given ongoing airborne transmission of the disease with explosive outbreaks described in congregate settings (3).
A global reduction in TB burden by 2035 to the levels envisaged by the WHO End TB Strategy will require a multifaceted approach to all forms of TB, as well as to latent infection (4, 5). In this article we summarise the global situation of drug-resistant TB using MDR/RR-TB as the main indicator and describe what is needed to mount an appropriate response to “roll back” the progression of this public health, and global health, security threat.
Background
The assessment of country-level, regional and global burden of disease and death attributed to MDR/RR-TB uses standardized surveillance and annual data collection from member states by the WHO Global TB Programme, described elsewhere (6). Burden of disease and attributable deaths are derived from empirical data updated annually from country mortality reports and vital registration systems, and from a comprehensive global TB drug resistance surveillance (DRS) programme established in 1994 (7, 8).
Since 1994, data on TB drug resistance have been systematically collected and analysed from 155 countries worldwide (80% of 194 WHO member states), which collectively have more than 95% of the world’s population and TB cases. This includes 83 countries that have continuous surveillance systems based on routine diagnostic drug-susceptibility testing (DST) of Mycobacterium tuberculosis isolates obtained from all TB patients, and 72 countries that rely on epidemiological surveys of bacterial isolates collected from representative samples of patients.
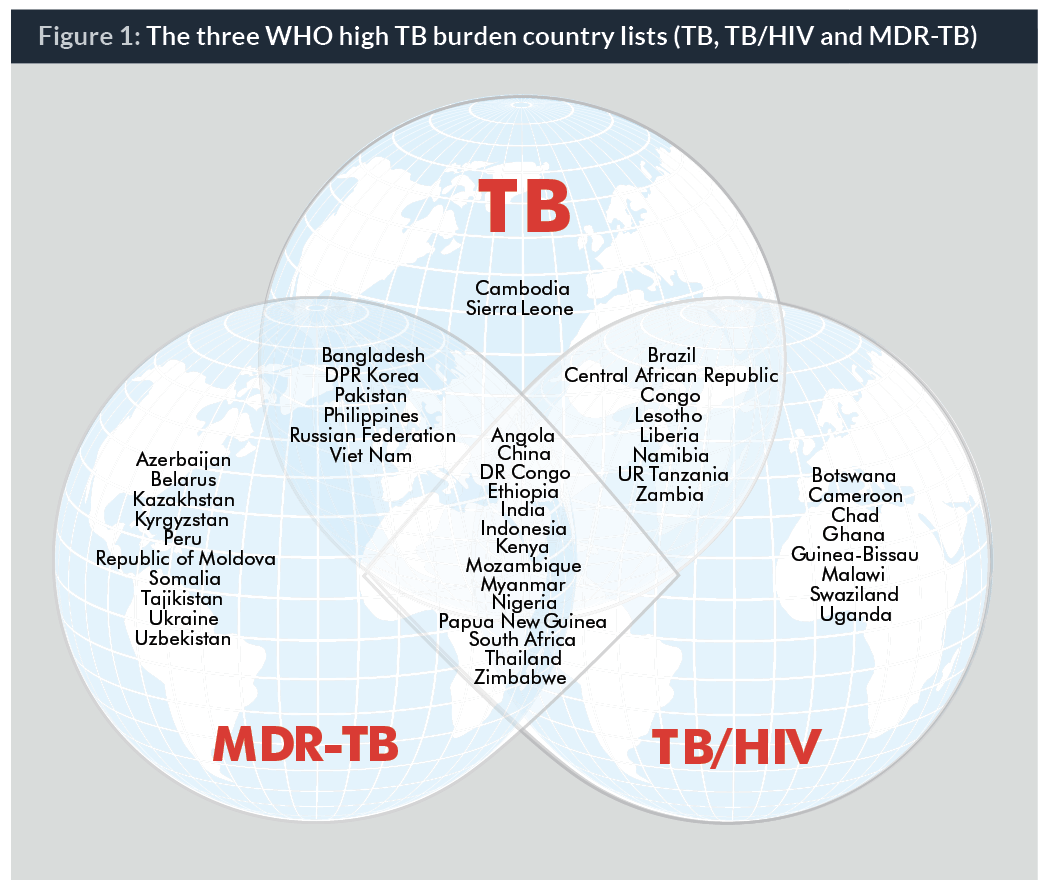
Trends in TB drug resistance have been tracked since 1994, together with targeted programmatic indicators such as diagnostic coverage, treatment enrolment, care delivery systems and treatment outcome. Data are available by country, and aggregated globally and by WHO region. Thirty countries responsible for 80% of the global MDR/RR-TB burden are targeted for specialized technical support to programmatic management of drug-resistant TB and for WHO monitoring and evaluation (9) (Figure 1).
Current status of the MDR/RR-TB epidemic and reasons why it remains a crisis
High burden of morbidity and mortality
The 2016 WHO Global TB Report indicated that there were 580,000 (range: 520,000–640,000) new cases of MDR/RR-TB in 2015 (2). An estimated 250,000 (160,000–340,000) MDR/RR-TB patients died in 2015.
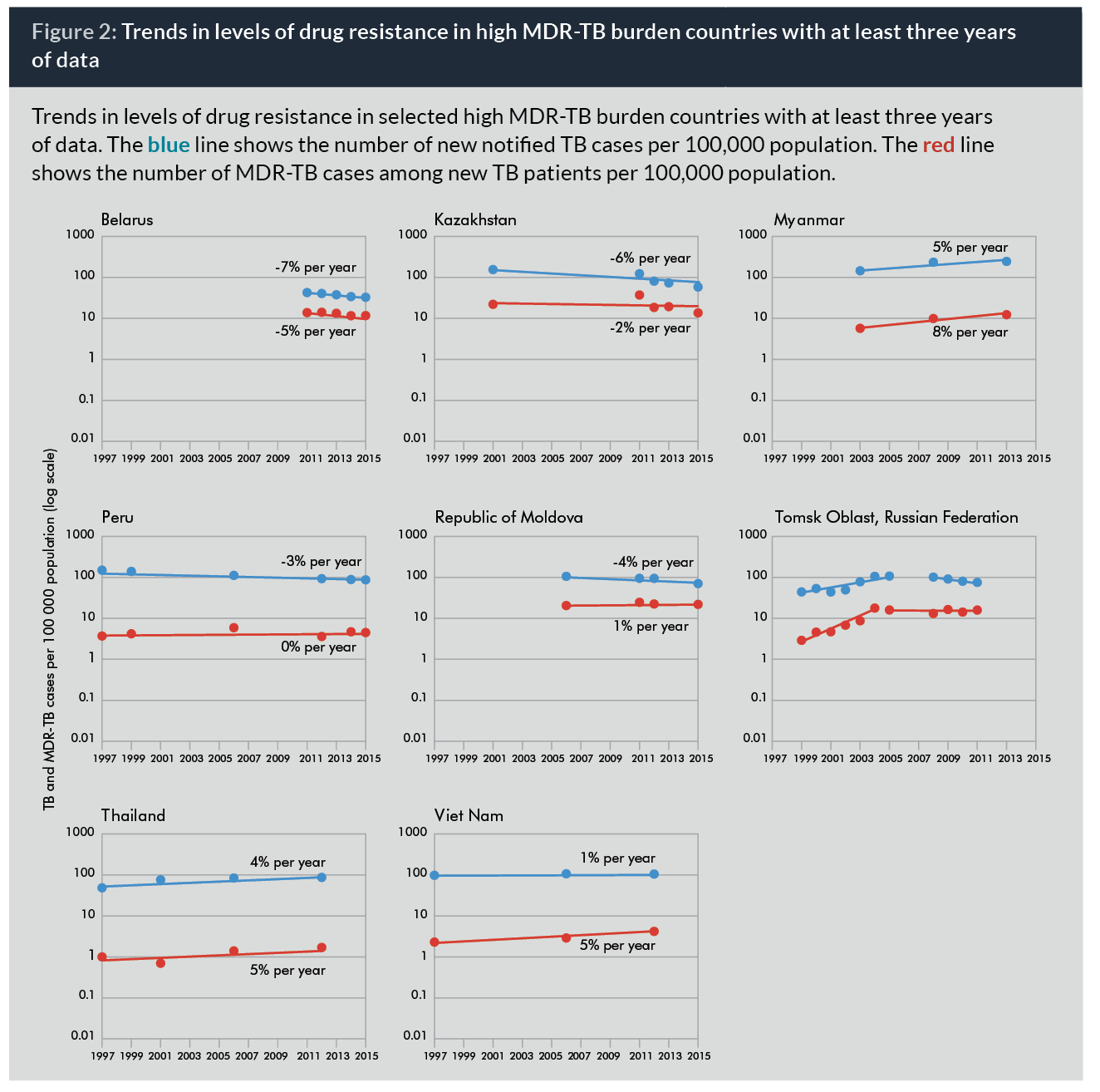
Drug resistance surveillance data show that globally, 3.9% (2.7-5.1%) of new and 21% (15-28%) of previously treated TB cases had MDR/RR-TB in 2015. Wide geographical and country variation occur, with China, Russia, India, South Africa, and some Asian and Eastern European countries carrying the heaviest MDR/RR-TB burden (10). Among countries with representative data for at least three years, the burden of MDR-TB is either increasing faster or decreasing more slowly than the overall TB burden, with a slight incremental trend in the number of MDR-TB cases as a proportion of all TB cases (Figure 2).
By the end of 2015, XDR-TB cases had been reported by 117 WHO member states. Over half of patients with MDR/RR-TB had additional resistance to either a fluoroquinolone or a second-line injectable agent or both. Pooled surveillance data show that 9.5% (7.0–12.1%) of MDR/RR-TB cases globally had XDR-TB, i.e. one in 10 patients had little treatment options left (and one in three of them died). Levels of XDR-TB are much higher than the global average in several countries of Eastern Europe and Central Asia (former USSR countries). Cases with resistance to most (if not all) available anti-TB medications have been reported from several settings in recent years (11-13).
Limited diagnostic coverage and treatment enrolment
The well-documented crisis of MDR/RR-TB detection and treatment continues unabated, with slow and limited uptake by countries of technological breakthroughs in diagnostics and treatment over the past 10 years. In 2015, only 24% of new and 53% of previously treated TB patients had drug susceptibility testing (DST) done, despite the 2009 World Health Assembly Resolution 62.15 on universal DST and treatment for all MDR-TB cases. The WHO European Region is the only part of the world where DST coverage has remained comparatively stable at a high level of 60–70%.
Globally, only around 20% of the 580,000 people newly eligible for second-line treatment in 2015 were detected and enrolled on treatment in 2015. This means 450,000 cases with MDR/RR-TB remained undiagnosed and untreated. Multiple reasons exist for the stagnation in detection and treatment of these patients (14); slow uptake of WHO-recommended rapid molecular diagnostics, access to, and cost of, second-line medicines, technical complexities in managing drug-resistant TB patients and health service weaknesses are common themes.
Poor treatment outcomes and significant health service challenges
Only 52% of 87,000 MDR/RR-TB patients who started second-line therapy in 2013 were reported by countries to have been successfully treated, while 17% of patients died, 22% were lost to follow-up or not evaluated and treatment failed in 9% of patients. Among over 4,000 XDR-TB patients started on treatment worldwide in 2013, only 28% completed treatment successfully, 27% died, treatment failed for 21%, and 23% were lost to follow-up or not evaluated. These outcomes have remained static despite improvements in the coverage of treatment and availability of more effective or new medicines, for example, later-generation fluoroquinolones, bedaquiline and delamanid.
Hospitalization of patients with MDR/RR-TB is still the predominant model of care in many countries despite WHO recommendations for a decentralised approach to treatment. Ten high-burden MDR-TB countries reported hospitalization for all MDR-TB patients in 2015, including two of the top three MDR-TB burden countries: China and the Russian Federation. In a further six high MDR-TB burden countries, at least 90% of MDR/RR-TB patients were hospitalized. In most of these countries the average length of stay was 160 days.
Hospitalization cost is one of the main drivers in the overall cost per patient treated in the high-burden TB countries, ranging from US$ 100–1,000 for drug-susceptible TB and US$ 2,000–20,000 for MDR/RR-TB.
Airborne transmission and inadequate infection prevention and control
MDR/RR-TB is by far the greatest and most serious drug-resistant airborne disease. Transmission occurs almost exclusively via the air to close contacts of such cases, often in congregate settings and in vulnerable groups such as those with HIV co-infection, migrants, healthcare workers, prisoners and miners, or in children. Contrary to earlier assumptions, acquisition of drug resistance does not necessarily lower the transmissibility or virulence of TB strains (15, 16). Explosive outbreaks of M/XDR-TB have been well described in the literature (3, 17). Moreover, modelling studies and recent publications from several countries clearly show that transmission is a much more important driver of outbreaks or undetected epidemics than previously thought (18–20).
Lack of appropriate airborne infection control measures, limited tracing of MDR/RR-TB contacts and lack of efficacious treatment for latent MDR/RR-TB infection further compound the problem (21-30). The risk of MDR-TB replacing drug-susceptible TB epidemics has been flagged in modelling studies and is not entirely implausible (31, 32).
Suboptimal investment in MDR/RR-TB management, research and development
The high cost of existing commodities (especially medicines) for MDR/RR-TB severely stretches already limited country resources, and far too little investment goes to much-needed social support systems for patients and building resilient health services able to deliver quality care.
The 2016 WHO Global Report showed that international donor funding for TB falls far short of donor contributions for HIV and malaria, despite the fact that TB is the top infectious cause of death worldwide. The latest data from the Organisation for Economic Co-operation and Development (OECD) creditor reporting system show totals of US$ 5.4 billion for HIV/AIDS, US$ 1.7 billion for malaria and US$ 0.7 billion for TB in 2014 (2). Despite being by far the largest external donor in TB (more than 80% of international resources come from this mechanism), the Global Fund to Fight AIDS, TB and Malaria – which is the major international donor for the three diseases – invests less than 20% of its funding in TB control (33).
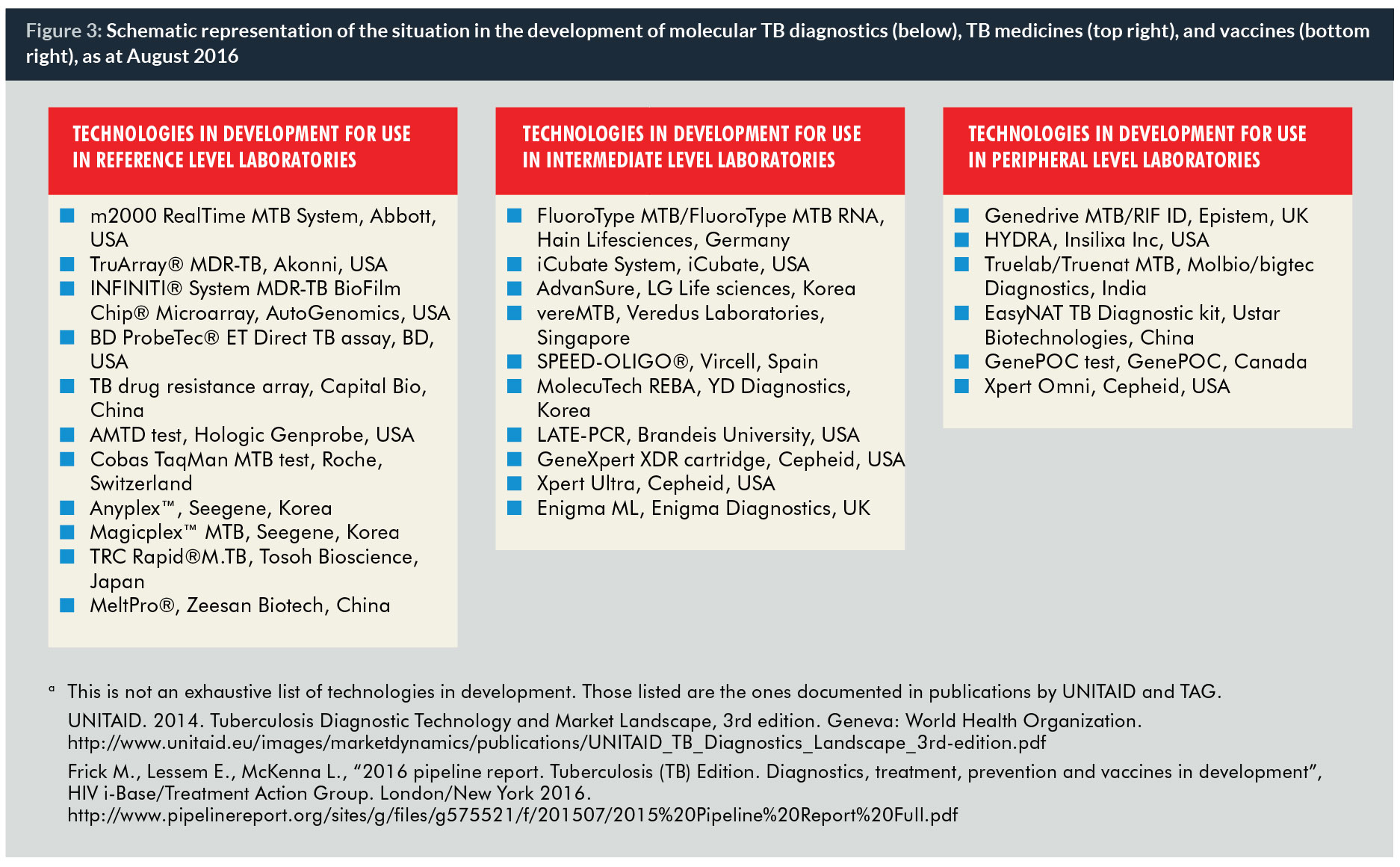
Research investment in developing transformational interventions for TB is also vastly insufficient. Funding for TB research and development is at its lowest level since 2008, at only US$ 620 million per year against the global estimated minimum annual need of at least US$ 2 billion (34). Funding during the decade 2005–2014 never exceeded US$ 0.7 billion per year, partly explaining the rather modest pipeline for new TB vaccines, medicines and, to a lesser extent, diagnostics (2) (Figure 3). In comparison, investment in anti-retroviral development has been many times more than in anti-TB agents, allowing more treatment options to be delivered to HIV patients in recent years.
Complacency and insufficient political commitment
Progress in response to the global MDR/RR-TB crisis is dismal. M/XDR-TB constitutes both a public health and international health security crisis which requires urgent, innovative and sustained interventions involving multiple state and non-state sectors. Unfortunately, the essential political will – which should translate into adequate financial and human resources to address the MDR/RR-TB crisis – is lacking in many countries, often those hardest hit by the epidemic. Complacency about TB as an “ancient” disease and reluctance by policy-makers to embrace innovations (notably rapid diagnostics and new drugs) threaten the strides made in TB control over the last ten years and poses a major barrier to containing and reversing the MDR/RR-TB crisis.
Discussion
The WHO End TB strategy is firmly positioned within the context of the post-2015 era of the Sustainable Development Goals (SDGs). Both the SDGs and the End TB Strategy share a common aim: to end the global TB epidemic and leave no-one behind. However, doing so will require an unprecedented acceleration in the rate at which TB incidence falls globally, together with an effective crisis response to contain the MDR/RR-TB epidemic while it is still possible.
The lethality of XDR-TB comes close to that observed among Ebola patients in the recent outbreaks in western Africa (2, 35). However, few realize that MDR-TB kills more than 10 times as many people every year as the entire last tragic Ebola epidemic. Poignantly, much of the MDR/RR-TB burden is man-made and largely preventable by curing patients without drug-resistant strains the first time around. Currently, only a few countries will achieve universal access to MDR/RR-TB care by 2025 should they sustain their current pace of progress. In most other countries a radical scale-up is needed to positively impact the MDR/RR-TB crisis and its devastating effects on patients and health services. Five priority actions have been identified by WHO to do so:
- Prevent the development of drug resistance through high-quality treatment of drug-susceptible TB;
- Expand rapid testing and detection of drug-resistant TB cases;
- Provide immediate access to effective treatment and proper care;
- Prevent transmission through proper infection control; and
- Increase political commitment and provide adequate financing.
Changing the course of the TB epidemic will require technological breakthroughs – for example, a post-exposure vaccine, short and efficacious treatment for latent TB infection, novel diagnostics to identify those at greatest risk of developing active disease once infected, and completely new, universal short treatment regimens that would be effective despite the presence of drug resistance. Accelerated uptake of emerging innovations such as digital health technologies (36, 37), combined with efforts to improve quality-of-life of people while on treatment, are equally important.
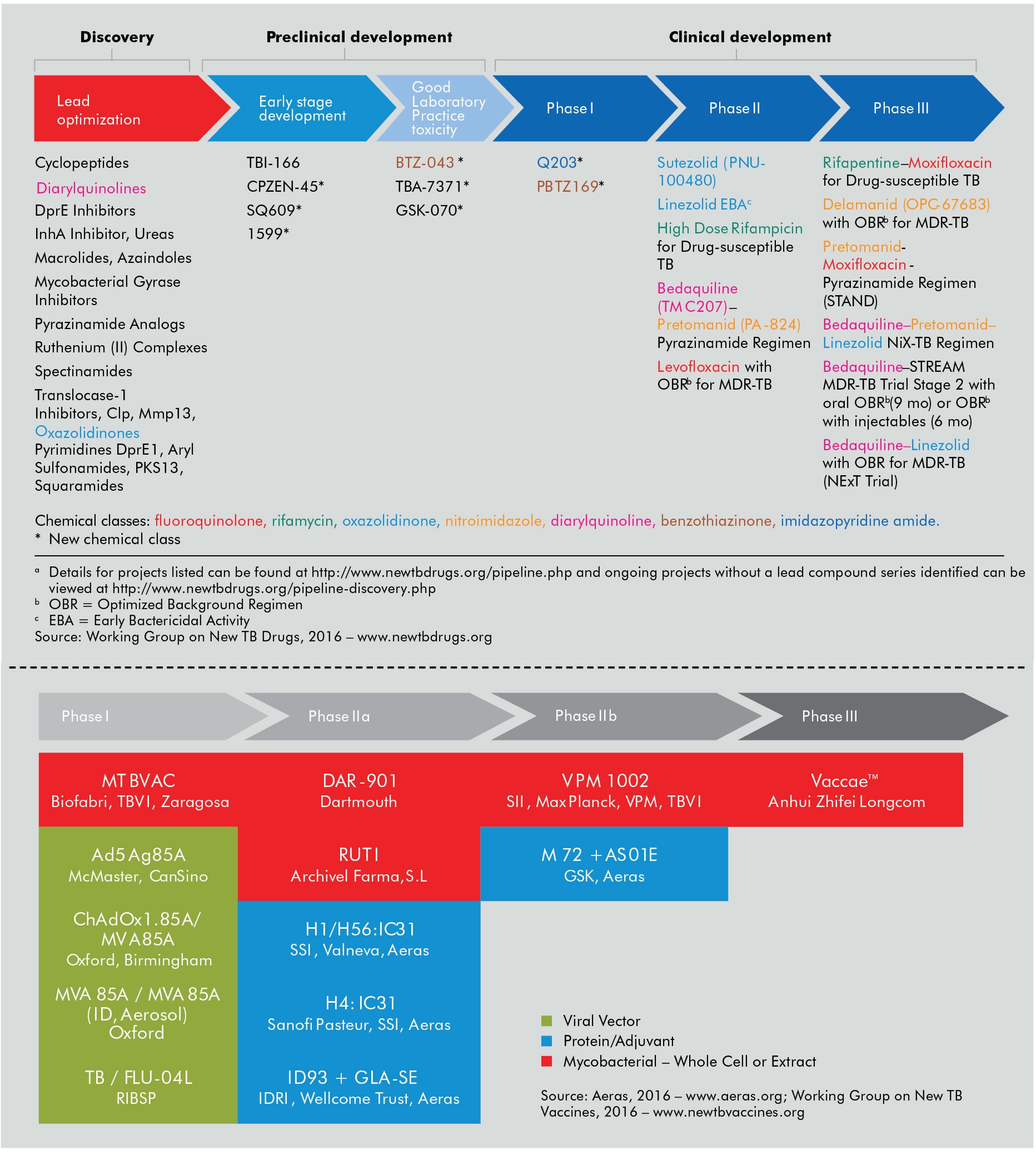
Some technological breakthroughs are already available and ready for immediate scale-up (Figure 4). WHO recommended four new diagnostic tests in 2016 alone – one of these being a rapid DNA-based line probe assay that identifies genetic mutations in MDR/RR-TB strains, providing results in 24–48 hours and helping to guide appropriate treatment regimens (38). Furthermore, bedaquiline and delamanid, the first completely new MDR/RR-TB drugs ever, were recommended by WHO in 2013 and 2014 respectively (39, 40). In 2016, WHO recommended a shorter, standardized treatment regimen for the majority of MDR/RR-TB patients, which could overcome several of the barriers faced by patients and health services in MDR/RR-TB care delivery (41, 42). Policy guidance on the shorter MDR-TB regimen also benefited from strategically targeted operational research, as shown recently (43).
Yet more innovations are at the door. Novel genome sequencing technologies could expand and refine surveillance of drug-resistant TB and, in the longer term, guide individual patient care (44, 45). Nine anti-TB drugs are currently in an advanced stage of development and 13 vaccine candidates are in clinical trials (2). Novel new regimens are under development and could potentially reach the market by 2020, the first milestone for measuring progress in the WHO End TB Strategy (46, 47).

Conclusions
The MDR/RR-TB crisis demonstrates many of the challenges that will be faced by broader AMR control efforts. The response to this challenge has shown that several critical elements are essential for the control of drug-resistant infectious diseases in countries. These include good quality surveillance, rapid diagnosis of drug resistance, appropriate treatment, improved infection prevention and control, and good care delivery systems with trained health personnel. Moreover, problems in treating MDR/RR-TB can point to a country or institution’s readiness to tackle AMR.
The AMR response at global and country level could greatly benefit from the challenges faced by TB care and control and by adopting some of TB’s “lessons learned”. Moreover, diagnostic platforms, logistics and digital technologies for sharing data can be used to link TB and AMR programmes at the country level. Existing regulatory frameworks, surveillance systems, infrastructure for laboratory services and infection control, and human resources already in place to manage drug resistance in tuberculosis, HIV and malaria could be additional resources to governments implementing AMR plans (48).
At the global level, at least two high-level initiatives present ample opportunity to address MDR/RR-TB within broader health agendas: the WHO Global Action Plan on Antimicrobial Resistance calls for inclusive, multisectoral and innovative partnerships to foster the development of antibiotics, responsible use of medicines, coordinated research and development of new drugs, diagnostics and vaccines (in close collaboration with industry), with strategies to ensure affordability and access for all. The Global Health Security Agenda (GHSA) is an effort between nations, international organizations and civil society to accelerate progress towards a world safe and secure from infectious disease threats and to promote global health security as a national and international priority (49).
Prominent space for the MDR/RR-TB crisis, enhanced linkages and increased collaboration within these global agendas is urgently needed. The upcoming WHO Ministerial Conference co-hosted by the Russia Federation in November 2017 and the planned 2018 United Nations General Assembly high-level meeting on TB (50, 51), will be key opportunities to firmly position MDR/RR-TB within the AMR and global health security agendas; secure political commitment and dedicated funding to tackle the MDR/RR-TB crisis; form strategic partnerships exerting enough pressure to reduce the cost of commodities; agree on a prioritized research agenda; and consider existing global measures such as the International Health Regulations to contain the M/XDR-TB crisis. Time and renewed political will are, however, of the essence.
Biographies
Dr Dennis Falzon, MD, is a Medical Officer with the Global TB Programme of the World Health Organization (WHO/GTB) in Switzerland. Until 2008, he coordinated the EuroTB surveillance project at the Institut de veille sanitaire in Paris, France and before that he worked in TB monitoring and treatment with Médecins Sans Frontières in Central Asia. His current work focuses on the WHO policy guidance for the treatment of drug-resistant tuberculosis (DR-TB), and also leading the drive of WHO/GTB to integrate more digital technologies in different components of the End TB Strategy.
Dr Ernesto Jaramillo, MD, PhD, is the team lead of the WHO Global TB Programme for DR-TB policies. He holds a degree in medicine and surgery at Universidad del Valle, Cali, Colombia and a PhD from University of London, London, UK. His entire career as clinician and in public health has been devoted to TB. Since 2001, he has been working at WHO in the development of policies for the management of DR-TB, covering a scope that includes treatment of MDR-TB, ethics, human rights, patient-centred care, pharmacovigilance and palliative care, among other areas of work.
Dr Matteo Zignol, MD, MPH, is the Team Lead of the World Health Organization Global Project on Anti-Tuberculosis Drug resistance Surveillance, based in Geneva, Switzerland. He joined the World Health Organization in 2003 and his main areas of work are: surveillance of drug-resistant tuberculosis; interactions between epidemics of HIV and multidrug-resistant tuberculosis; management of drug-resistant tuberculosis; global policies to address multidrug-resistant and extensively drug-resistant tuberculosis; and operations research on drug-resistant tuberculosis. He is an infectious disease specialist and clinical epidemiologist. He holds a MD from the University of Padua, Italy, and a MPH from Johns Hopkins University, Baltimore, US.
Dr Fuad Mirzayev leads the team on Policy Transfer and Uptake of the WHO Global TB Programme Unit for Laboratories, Diagnostics and Drug Resistance (LDR). He holds a degree in medicine from the State Medical University of Azerbaijan and MPH from the School of Public Health and Tropical Medicine at Tulane University, USA. He joined the World Health Organization in 2004 and his main areas of work included management of drug-resistant tuberculosis and access to second line anti-TB medicines via Green Light Committee Initiative; coordination of multi-country projects to expand access to innovative TB diagnostics. Prior to joining WHO he has worked for the International Committee of the Red Cross with its pioneer TB Control programme in penitentiary systems of countries in transition.
Professor Mario C Raviglione, MD, has been Director of the Global TB Programme at WHO since 2003. He was part of the team that developed the DOTS strategy in 1994, and set up the global drug-resistance surveillance project (1994) and the global TB surveillance and monitoring system (1995). He directed the teams who developed the latest global strategies: Stop TB in 2006 and End TB in 2014. As a leading expert in TB, he has worked in over 50 countries worldwide. He has served as a visiting professor at Johns Hopkins University, Université de Genève, Università di Modena; Reggio Emilia, Università di Pavia and University of Brescia where he is professor. He has published over 350 articles and book chapters, and he is among the top 10 most cited authors in the TB field. He is editor of the 3rd and 4th (2006, 2009) editions of Tuberculosis – A comprehensive International Approach. He graduated from the University of Turin in Italy in 1980, and trained in internal medicine and infectious diseases in New York (where he was Chief Medical Resident at Cabrini’s Medical Centre) and Boston, where he was an AIDS Clinical Research Fellow at Beth Israel Hospital, Harvard Medical School. In 2005, he received the Princess Chichibu TB Global Award for his achievements in TB control.
References
1. Antimicrobial drug resistance. Report by the Secretariat. A67/39. Geneva, World Health Organization; 2014. Available from: http://apps.who.int/gb/ebwha/pdf_files/WHA67/A67_39-en.pdf
2. Global tuberculosis report 2016 (WHO/HTM/TB/2016.13). Geneva, World Health Organization; 2016. Available from: http://apps.who.int/iris/bitstream/10665/250441/1/9789241565394-eng.pdf
3. Gandhi NR, Moll A, Sturm AW, Pawinski R, Govender T, Lalloo U, et al. Extensively drug-resistant tuberculosis as a cause of death in patients co-infected with tuberculosis and HIV in a rural area of South Africa. Lancet. 2006 Nov 4;368(9547):1575–80.
4. Uplekar M, Weil D, Lönnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. WHO’s new end TB strategy. Lancet. 2015 May 2;385(9979):1799–801.
5. Implementing the End TB Strategy: the essentials (WHO/HTM/TB/2015.31). Geneva, World Health Organization. 2015. Available from: http://www.who.int/tb/publications/2015/end_tb_essential.pdf
6. Technical Appendix – Methods used to estimate the global burden of disease caused by TB in Global tuberculosis report 2014 (available online only). Geneva, World Health Organization. 2014. Available from: http://www.who.int/tb/publications/global_report/gtbr14_online_technical_appendix.pdf
7. Zignol M, Dean AS, Falzon D, van Gemert W, Wright A, van Deun A, et al. Twenty years of global surveillance of antituberculosis-drug resistance. New Eng J Med. 2016 Sep 15;375(11):1081–9.
8. WHO Mortality Database. Available from: http://www.who.int/healthinfo/mortality_data/en/
9. Use of high burden country lists for TB by WHO in the post-2015 era (WHO/HTM/TB/2015.29). 2015. Available from: http://www.who.int/tb/publications/global_report/high_tb_burdencountrylists2016-2020.pdf
10. Falzon D, Mirzayev F, Wares F, Baena IG, Zignol M, Linh N, et al. Multidrug-resistant tuberculosis around the world: what progress has been made? Eur Respir J. 2015 Jan 1;45(1):150–60.
11. Migliori GB, De Iaco G, Besozzi G, Centis R, Cirillo DM. First tuberculosis cases in Italy resistant to all tested drugs. Euro Surveill. 2007 May;12(5):E070517.1.
12. Velayati AA, Masjedi MR, Farnia P, Tabarsi P, Ghanavi J, Ziazarifi AH, et al. Emergence of new forms of totally drug-resistant tuberculosis bacilli: super extensively drug-resistant tuberculosis or totally drug-resistant strains in Iran. Chest. 2009 Aug;136(2):420–5.
13. Udwadia ZF, Amale RA, Ajbani KK, Rodrigues C. Totally drug-resistant tuberculosis in India. Clin Infect Dis. 2012 Feb 15;54(4):579–81.
14. Médecins Sans Frontières, Stop TB Partnership. Out of Step 2015. TB Policies in 24 Countries. A survey of diagnostic and treatment practices. Geneva, Switzerland; 2015. Available from: http://www.msfaccess.org/sites/default/files/MSF_assets/TB/Docs/TB_report_Out_of_Step_ENG_2015.pdf
15. Gagneux S. Fitness cost of drug resistance in Mycobacterium tuberculosis. Clinical Microbiology and Infection. 2009 Jan;15:66–8.
16. Borrell S, Gagneux S. Infectiousness, reproductive fitness and evolution of drug-resistant Mycobacterium tuberculosis. Int J Tuberc Lung Dis. 2009 Dec;13(12):1456–66.
17. Frieden TR, Sherman LF, Maw KL, Fujiwara PI, Crawford JT, Nivin B, et al. A multi-institutional outbreak of highly drug-resistant tuberculosis: epidemiology and clinical outcomes. JAMA. 1996 Oct 16;276(15):1229–35.
18. Kendall EA, Fofana MO, Dowdy DW. Burden of transmitted multidrug resistance in epidemics of tuberculosis: a transmission modelling analysis. The Lancet Respiratory Medicine. 2015 Dec;3(12):963–72.
19. Shah NS, Auld SC, Brust JCM, Mathema B, Ismail N, Moodley P, et al. Transmission of Extensively Drug-Resistant Tuberculosis in South Africa. New England Journal of Medicine. 2017 Jan 19;376(3):243–53.
20. Leung ECC, Leung CC, Kam KM, Yew WW, Chang KC, Leung WM, et al. Transmission of multidrug-resistant and extensively drug-resistant tuberculosis in a metropolitan city. Eur Respir J. 2013 Apr;41(4):901–8.
21. Schaaf HS, Gie RP, Kennedy M, Beyers N, Hesseling PB, Donald PR. Evaluation of young children in contact with adult multidrug-resistant pulmonary tuberculosis: a 30-month follow-up. Pediatrics. 2002 May;109(5):765–71.
22. Kritski AL, Marques MJ, Rabahi MF, Vieira MA, Werneck-Barroso E, Carvalho CE, et al. Transmission of tuberculosis to close contacts of patients with multidrug-resistant tuberculosis. Am J Respir Crit Care Med. 1996 Jan;153(1):331–5.
23. Attamna A, Chemtob D, Attamna S, Fraser A, Rorman E, Paul M, et al. Risk of tuberculosis in close contacts of patients with multidrug resistant tuberculosis: a nationwide cohort. Thorax. 2009 Mar 1;64(3):271–271.
24. Denholm JT, Leslie DE, Jenkin GA, Darby J, Johnson PDR, Graham SM, et al. Long-term follow-up of contacts exposed to multidrug-resistant tuberculosis in Victoria, Australia, 1995–2010. Int J Tuberc Lung Dis. 2012 Oct 1;16(10):1320–5.
25. Trieu L, Proops DC, Ahuja SD. Moxifloxacin Prophylaxis against MDR TB, New York, New York, USA. Emerging Infectious Diseases. 2015 Mar;21(3):500–3.
26. Garcia-Prats AJ, Zimri K, Mramba Z, Schaaf HS, Hesseling AC. Children exposed to multidrug-resistant tuberculosis at a home-based day care centre: a contact investigation. Int J Tuberc Lung Dis. 2014 Nov 1;18(11):1292–8.
27. Bamrah S, Brostrom R, Dorina F, Setik L, Song R, Kawamura LM, et al. Treatment for LTBI in contacts of MDR-TB patients, Federated States of Micronesia, 2009–2012. Int J Tuberc Lung Dis. 2014 Aug 1;18(8):912–8.
28. Adler-Shohet FC, Low J, Carson M, Girma H, Singh J. Management of Latent Tuberculosis Infection in Child Contacts of Multidrug-Resistant Tuberculosis: The Pediatric Infectious Disease Journal. 2014 Jun;33(6):664–6.
29. Fox GJ, Anh NT, Nhung NV, Loi NT, Hoa NB, Ngoc Anh LT, et al. Latent tuberculous infection in household contacts of multidrug-resistant and newly diagnosed tuberculosis. Int J Tuberc Lung Dis. 2017 Mar 1;21(3):297–302.
30. Shenoi SV, Escombe AR, Friedland G. Transmission of drug-susceptible and drug-resistant tuberculosis and the critical importance of airborne infection control in the era of HIV infection and highly active antiretroviral therapy rollouts. Clin Infect Dis. 2010 May 15;50 Suppl 3:S231-237.
31. McBryde ES, Meehan MT, Doan TN, Ragonnet R, Marais BJ, Guernier V, et al. The risk of global epidemic replacement with drug-resistant Mycobacterium tuberculosis strains. International Journal of Infectious Diseases. 2017 Mar;56:14–20.
32. Dye C, Williams BG, Espinal MA, Raviglione MC. Erasing the world’s slow stain: strategies to beat multidrug-resistant tuberculosis. Science. 2002 Mar 15;295(5562):2042–6.
33. About the Global Fund to Fight AIDS, Tuberculosis and Malaria – The Global Fund to Fight AIDS, Tuberculosis and Malaria. Available from: http://www.theglobalfund.org/en/about/
34. Treatment Action Group. 2016 Report on Tuberculosis Research Funding Trends, 2005–2015: No Time to Lose. 2016. Available from: http://www.treatmentactiongroup.org/sites/default/files/TB_FUNDING_2016_WEB.pdf
35. Ebola data and statistics. Available from: http://apps.who.int/gho/data/view.ebola-sitrep.ebola-summary-latest?lang=en
36. Implementing tuberculosis diagnostics: A policy framework (WHO/HTM/TB/2015.11). Geneva, World Health Organization. 2015. Available from: http://apps.who.int/iris/bitstream/10665/162712/1/9789241508612_eng.pdf
37. WHO/ERS. Digital health for the End TB Strategy: an agenda for action. (WHO/HTM/TB/2015.21). Geneva, World Health Organization; 2015. Available from: http://apps.who.int/iris/bitstream/10665/205222/1/WHO_HTM_TB_2015.21_eng.pdf
38. The use of molecular line probe assays for the detection of resistance to second-line anti-tuberculosis drugs. Policy guidance. (WHO/HTM/TB/2016.07). Geneva, World Health Organization. 2016. Available from: http://www.who.int/tb/publications/lpa-mdr-diagnostics/en/
39. The use of bedaquiline in the treatment of multidrug-resistant tuberculosis. Interim policy guidance (WHO/HTM/TB/2013.6). Geneva, World Health Organization. 2013. Available from: http://apps.who.int/iris/bitstream/10665/84879/1/9789241505482_eng.pdf
40. The use of delamanid in the treatment of multidrug-resistant tuberculosis. Interim policy guidance (WHO/HTM/TB/2014.23). Geneva, World Health Organization. 2014. Available from: http://apps.who.int/iris/bitstream/10665/137334/1/WHO_HTM_TB_2014.23_eng.pdf
41. WHO treatment guidelines for drug-resistant tuberculosis, 2016 update (WHO/HTM/TB/2016.04). Geneva, World Health Organization. 2016. Available from: http://apps.who.int/iris/bitstream/10665/250125/1/9789241549639-eng.pdf
42. Falzon D, Schünemann HJ, Harausz E, González-Angulo L, Lienhardt C, Jaramillo E, et al. World Health Organization treatment guidelines for drug-resistant tuberculosis, 2016 update. Euro Respir J. 2017 Mar;49(3):1602308.
43. Yassin MA, Jaramillo E, Wandwalo E, Falzon D, Scardigli A, Kunii O, et al. Investing in a novel shorter treatment regimen for multidrug-resistant tuberculosis: to be repeated. European Respiratory Journal. 2017 Mar;49(3):1700081.
44. Walker TM, Merker M, Kohl TA, Crook DW, Niemann S, Peto TEA. Whole genome sequencing for M/XDR tuberculosis surveillance and for resistance testing. Clin Microbiol Infect. 2017 Mar;23(3):161–6.
45. Votintseva AA, Bradley P, Pankhurst L, Del Ojo Elias C, Loose M, Nilgiriwala K, et al. Same-day diagnostic and surveillance data for tuberculosis via whole genome sequencing of direct respiratory samples. J Clin Microbiol. 2017 Mar 8;
46. Tuberculosis Medicines Technology and Market Landscape. UNITAID, Geneva; 2013 [cited 2017 Mar 30]. Available from: http://unitaid.org/images/marketdynamics/publications/UNITAID-TB_Medicines_Landscape-1st_edition.pdf
47. Our Pipeline | TB Alliance. Available from: http://w.pdpaccess.org/pipeline/pipeline.php
48. WHO | WHO publishes list of bacteria for which new antibiotics are urgently needed. Available from: http://www.who.int/mediacentre/news/releases/2017/bacteria-antibiotics-needed/en/
49. Home | Global Health Security Agenda. Available from: https://www.ghsagenda.org/
50. PRESS RELEASE: High-Level Meeting on Antimicrobial Resistance | General Assembly of the United Nations [Internet]. [cited 2016 Nov 7]. Available from: http://www.un.org/pga/71/2016/09/21/press-release-hl-meeting-on-antimicrobial-resistance/
51. WHO | UN General Assembly high-level meeting on TB to take place in 2018. Available from: http://www.who.int/tb/features_archive/unga-meeting-tuberculosis/en/



{kind=link}