Molly Miller-Petrie Research Associate, CDDEP and Hellen Gelband, Associate Director for Policy, CDDEP
Global patterns of health and disease vary by national economic status, and individual health and healthcare are also heavily influenced by family social and economic status within countries. It is no surprise that the levels and patterns of antimicrobial resistance – which reflect disease incidence and antimicrobial use patterns – also vary around the globe (1-4). Because socioeconomic factors have been directly linked to antimicrobial use, and use drives antimicrobial resistance (AMR), socioeconomic factors can be considered indirect drivers of AMR.
At a societal level, disease burden, health system development, pharmaceutical regulations and enforcement, health insurance or national healthcare coverage, and access to and quality of medicines all affect antimicrobial use and are affected by socioeconomic factors. Individuals, both high- and low-income, operate in their own societal conditions, and their individual behaviour also impacts patterns of antimicrobial use and ultimately, resistance. Drug-resistant infections also affect patients’ social and economic status by increasing healthcare costs, mortality and morbidity, and decreasing productivity.
In this article, we review the evidence for socioeconomic effects on antimicrobial use and AMR at global, national, and individual levels. We consider human health, animal health and agriculture, and the environment – following the One Health concept.
Global-level economic correlates of AMR and antimicrobial use
Low- and many middle-income countries (LMICs) face relatively higher rates of infectious diseases, in part due to geography and in part because of limited preventive medical and environment services, particularly sanitation and clean water. Resistant bacteria have been detected at higher rates in urban compared to rural areas (5). Poor public health, including shortfalls in immunization, infection prevention and control, and piped water, sanitation and hygiene, further contribute to the disease burden in LMICs. Effective treatment is hampered by weak and under-resourced health systems in many countries. Minimal or nonexistent regulations governing antimicrobial use and production and an absence of surveillance systems to track and respond to emerging disease threats further compound these issues.
Documenting rates of AMR and antimicrobial use
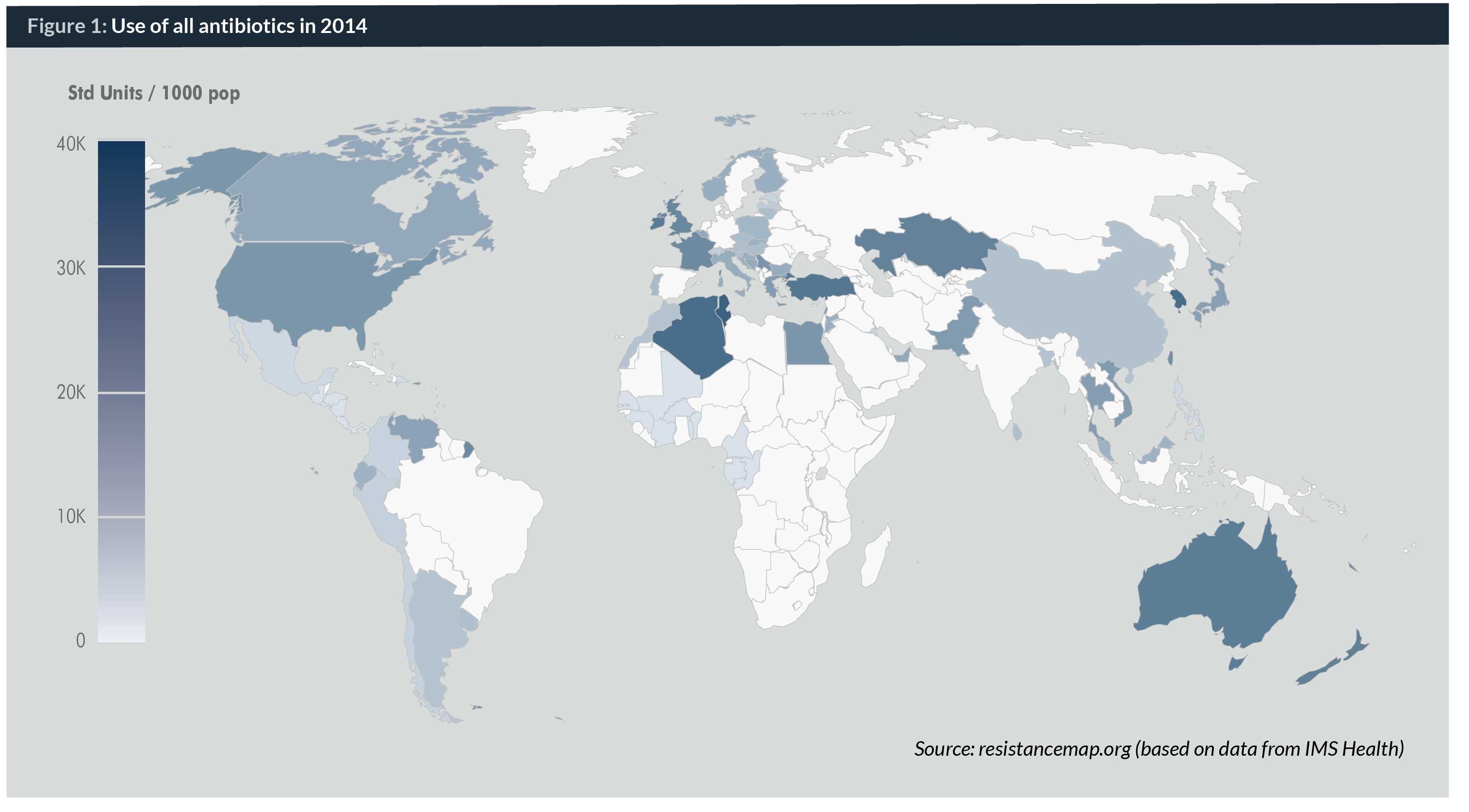
A striking manifestation of an effect of national economic status on AMR is the paucity of data on the levels and patterns of antimicrobial use and AMR in LMICs. Global repositories, including ResistanceMap – the largest such database – have gaps in data for parts of Africa, Asia and Latin America (Maps 1 and 2). Globally, the best available data are for Europe (through the European Antimicrobial Resistance Surveillance Network (EARS–Net) and other high-income regions.
Several middle-income countries, particularly in the Pan American Health Organization (PAHO) region, have contributed AMR data to the Latin American Antibiotic Resistance Surveillance Network (ReLAVRA), and other networks, including the Asian Network for Surveillance of Resistant Pathogens (ANSORP), and the Central Asian and Eastern European Surveillance of Antimicrobial Resistance Network (CAESAR). Some LMICs, including Cambodia, Malaysia, Micronesia, Mongolia, the Philippines, South Africa and Thailand have national surveillance programmes in place (6, 7), but the situation is poorly documented, if at all, in most low-income countries.
The lack of AMR data in LMICs does not stem only from the lack of surveillance systems to gather test data from hospitals and laboratories. A fundamental problem is the very limited microbiology testing in low-income countries, as illustrated by an evaluation of a World Bank-supported clinical laboratory network in East Africa in 2016 (15). Even after substantial investments in buildings and equipment, few antimicrobial susceptibility tests were conducted. The reasons included stock-outs of consumables, as might be expected, but equally important is the fact that physicians rarely requested bacterial cultures or susceptibility testing prior to initiation of antimicrobial treatment. The reasons are many. Firstly, a lack of appreciation for the value of these test results – which may be justified in many cases because of the poor quality of testing, related to stock-outs and inadequate quality control. Secondly, results may take at least two days, by which time patients may be gone from the hospital. And thirdly, patients must pay for laboratory tests directly in most of the countries represented (which is common in other low-income countries), and physicians are reluctant to incur this cost to patients, especially in light of their lack of trust in the results.
The most comprehensive and detailed data on antimicrobial use comes from the European Surveillance of Antimicrobial Consumption Network (ESAC–Net), which began collating comprehensive information on annual antimicrobial use in the community and acute-care hospitals in Europe in 2011. The most recent ESAC–Net report, from 2012, includes 28 EU member states and two EEA countries (Iceland and Norway) (8). Countries gather data from sales and from reimbursement databases, and include product-level information. For the United States, which has no comparable system, the best data from which to estimate use come from IMS Health, a private data aggregator. IMS also collects data in Europe and a number of LMICs (Map 1).
Antimicrobial resistance
Few studies have attempted to directly correlate socioeconomic factors with national resistance rates. One such study found that resistance rates for three important bacteria: Escherichia coli, 3GC-resistant Klebsiella, and methicillin-resistant Staphylococcus aureus (MRSA), decreased as gross national income (GNI) per capita increased (9). However, GNI did not account for all of the variation in rates detected between income groups, and for S. aureus it accounted for less than half.
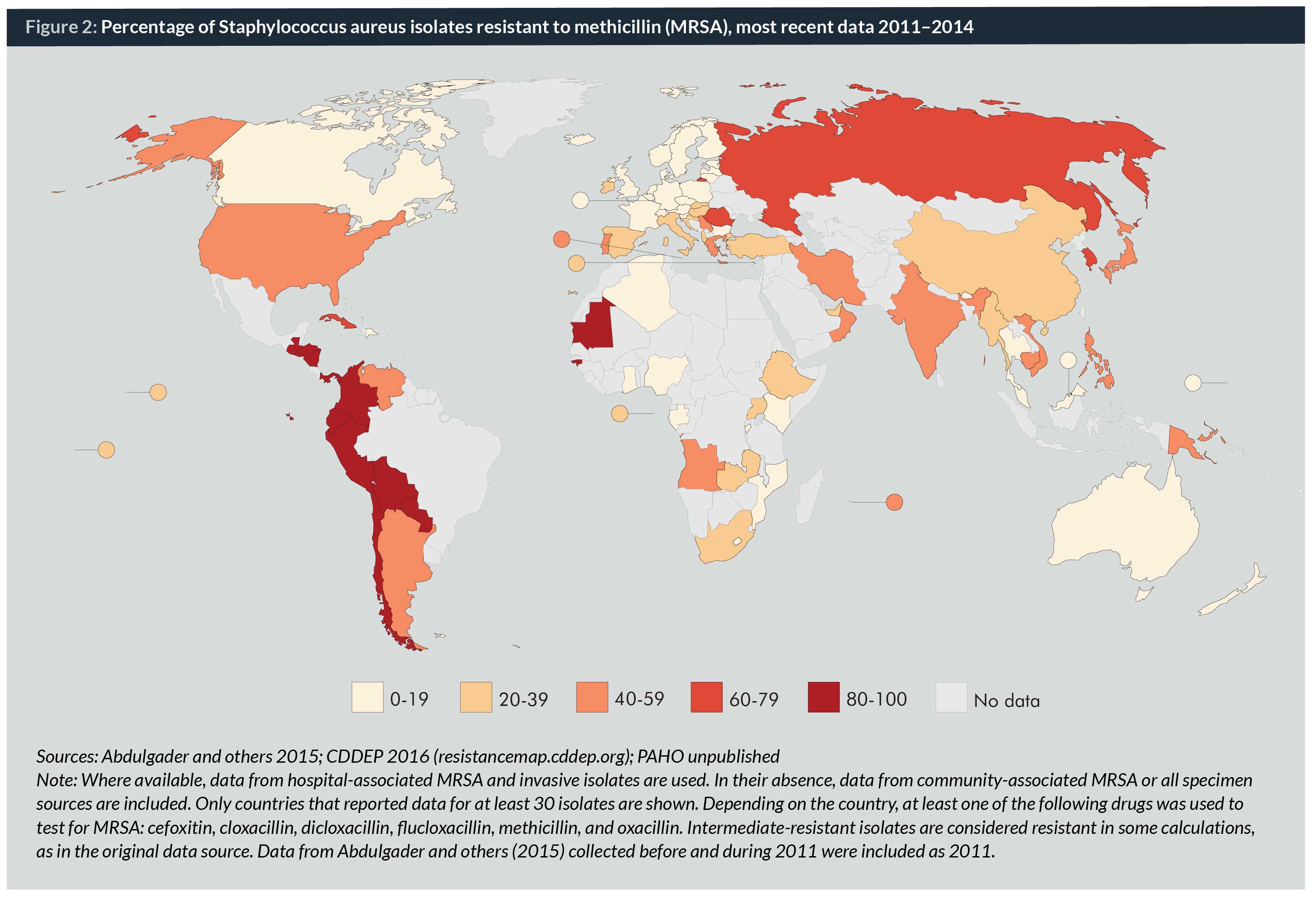
Countries within the same income group have highly variable rates of resistance. For example, according to the most recent data available, rates of MRSA were higher in the United States (44%) than in Australia (18%), Canada (16%), and the EU (17%). Rates in the EU varied from a low of 0% in Iceland to a high of 57% in Romania (Map 2 and Table 1) (10–12).
Reported rates of MRSA from LMICs are often derived from fewer isolates and may not be as reliable as those from high-income countries (HICs). Reported MRSA rates were over 80% in parts of West Africa and in much of Latin America, and over 40% in much of South and Southeast Asia (Map 2 and Table 1)(10,13,14), but questions remain about the reliability and comparability of these rates.
Resistance rates for several antimicrobial-pathogen combinations are higher and increasing faster in LMICs than in HICs (Map 2) (10).
Antimicrobial use
In general, HICs use more antimicrobials per capita than LMICs (15), but rates of antimicrobial consumption are increasing the fastest in LMICs (16). Antimicrobial use in animals is also increasing in many LMICs, in response to rising incomes and increased consumer demand for animal protein (17). Some HICs, particularly in Europe, have reduced their antimicrobial consumption after introducing limits on the use of antimicrobials to promote growth in animals, while others, such as Germany and the United States, were among the top consumers of antimicrobials in agriculture in 2010.
Among countries where use has been successfully reduced, significant investments were necessary to improve biosafety and biosecurity on farms in order to enable intensive production systems without the use of antimicrobials. Similar measures could be implemented in newer facilities in LMICs but may be too expensive for small livestock operations that lack the necessary technical and financial resources. Regardless, the benefits of reducing national resistance rates are predicted to outweigh the costs of introducing such bans. One study predicted that a worldwide ban on antimicrobial growth promoters would lead to a decrease of 1% to 3% in global meat production and a loss in meat production value of US$ 13.5 to US$ 44.1 billion, compared to an estimated loss of US$ 35 billion per year in the United States alone due to healthcare costs and losses to productivity from AMR (18, 19).
Regulation of antimicrobials in LMICs
In HICs, the mere promulgation of laws and regulations has not solved all the problems related to antimicrobials – in particular, their overuse – as healthcare providers may still prescribe inappropriately. However, laws and regulations do restrict use and have a positive effect on the quality of products sold (20). LMICs may record the same types of legal constraints on paper, but enforcement is often lax to nonexistent. Whether the laws and regulations do not exist or are just not enforced, the result is the same: widespread over-the-counter antimicrobial sales without prescription (21) and widespread substandard and counterfeit products in most low-income countries and many middle-income countries (22, 23). Both of these conditions can lead to poor treatment outcomes, higher rates of inappropriate antimicrobial use, and ultimately AMR.
Over-the-counter sales of antimicrobials can be seen as a symptom of an under-resourced and inadequate primary healthcare infrastructure. Real and perceived lack of access to affordable public healthcare can drive consumers to bypass consultation with a provider because of geographical lack of access, the time lost in seeking care, or the price of even “free” care (5, 24-26). People may approach a pharmacist in a standard pharmacy, which may supply high-quality products, a drug shop, where they are unlikely to encounter a trained pharmacist, or a roadside or market drug seller. Until real access improves in a country, this array of antimicrobial sellers is unlikely to change.
The issue of drug quality is also correlated with national economic status. HICs tend to record few instances of substandard or counterfeit drugs entering the market (20) compared to countries lacking regulations and enforcement, where substandard medicines are a more common problem (22). India, Myanmar, and Nigeria have the most reported cases of substandard or counterfeit antibacterial agents in the literature (23). In addition to quality when a product leaves the factory, packaging and storage can lead to degraded products, especially in hot, humid conditions (23).
In recent years, it has also come to light that the lack of enforced environmental regulations has consequences for AMR. Massive antimicrobial residues in wastewater have been measured in the outflow from certain manufacturing plants in India (27).
Within-country socioeconomic patterns
Within countries, patterns of antimicrobial use can vary between socioeconomic strata as much as they do between nations. Socioeconomic characteristics of individuals, families and regions influence patient and provider interactions, ultimately affecting antimicrobial use and AMR. Both physicians and patients influence patterns of use, which vary by some socioeconomic characteristics of areas and of individuals and families.
The relationship between socioeconomic status (SES) and antimicrobial use is easier to study than SES and AMR. However, even the literature linking SES to antimicrobial use is limited and includes few studies from the last decade, when general knowledge of and attitudes toward antimicrobials have changed significantly. Very little is known from within LMICs, following the pattern that characterizes information availability for this subject generally.
Consumption of healthcare, including antimicrobials, is influenced heavily by cost to the consumer, and the most widespread and influential driver of consumer cost is health insurance or national healthcare coverage (28–30). The populations of almost all HICs (with the notable exception of the United States) are insulated from the full costs of healthcare through such coverage, so their consumption does not follow the supply and demand patterns of other commodities – wealthier individuals are not necessarily more likely to consume more. The story is different in LMICs, where out-of-pocket spending and opportunity costs associated with healthcare access can be high enough to drive families into poverty, even in countries where public facilities provide care that should be free.
The cost of drugs and a patient’s ability to pay for them influence how much and what healthcare providers choose to prescribe. In the United States, a free antimicrobials programme launched in 2006 resulted in higher rates of prescribing, particularly for drugs covered by the programme (31), and in Hungary in 2003, populations with access to free medicines and with higher levels of social assistance had higher rates of antimicrobial consumption (32).
Healthcare provider behaviour plays a major role in antimicrobial use. Providers are influenced in several ways: by financial incentives where physicians or their institutions profit directly from antimicrobial sales, patient pressure or demand for antimicrobials, and even by the time of day – “decision fatigue” may set in later in the day (33–35). In hospitals in both LMICs and HICs, healthcare providers tend to prescribe empirically and are unlikely to change or discontinue an antimicrobial treatment once initiated. In a study in six large hospitals in the United States, less than two-thirds of patients received appropriate cultures, and 66% of patients had no change to their antimicrobial treatment after five days, though 58% of patients had negative cultures (36). Other factors related to SES, such as a patient’s race, may also influence how a provider chooses to prescribe. In the United States in 2009, it was found that African American children were less likely than nonblack children to receive antimicrobials for a diagnosis that indicated the need for antimicrobial treatment (37).
One relationship that has been reported consistently is higher healthcare utilization rates in areas with higher concentrations of physicians. Higher rates of antimicrobial prescribing result from this, reinforcing the role that access to antimicrobials plays in determining rates of use (1). In a recent study in the United States, antimicrobial prescribing was higher when physician and clinic density were greater and clinics and retail points of access are generally concentrated in wealthier areas. The number of doctor’s visits per person is also higher in wealthier areas (4), leading to higher antimicrobial prescription rates, at least in HICs where this has been studied.
Self-medication with antimicrobials is also influenced by SES. In a recent study in the Middle East, individuals with lower incomes and education levels (21, 26) were more likely to self-medicate with non-prescription, leftover or shared antimicrobials. In Nigeria, individuals with lower education were also more likely to self-medicate with antimicrobials (38).
Wealthier individuals enjoy greater access to and choice among drugs, including new, last-resort treatments that are the most expensive and which may be unaffordable for lower income individuals. However, individual wealth is still limited by the overall national context that person lives within. High-income individuals in LMICs face more limited access to quality drugs compared to high-income individuals in HICs.

Conclusions
and AMR and its drivers are no exception. From the lack of documentation about AMR and antimicrobial use at the global level, to the economics of national healthcare budgets in high- and low-income countries, down to the individual pocketbooks of rich and poor individuals, access to effective antimicrobials at the appropriate time is influenced heavily by social and economic factors. Many of the published studies are more than a decade old and may not reflect the current relationships. The past decade has seen changes in attitudes towards antimicrobial use and in practices, to a greater extent in some countries than in others, with the degree and type of change associated closely with social norms and financial resources. Closing gaps associated with socioeconomic differences should figure more prominently in the current AMR and antimicrobial use agenda.
Biographies
Hellen Gelband is Associate Director for Policy at the Center for Disease Dynamics, Economics & Policy, where she directs the Global Antibiotic Resistance Partnership (GARP). She is also an editor of Disease Control Priorities 3rd edition and an editor with the Cochrane Collaboration Infectious Diseases Group.
References
1. Filippini M, Masiero G, Moschetti K. Socioeconomic determinants of regional differences in outpatient antibiotic consumption: evidence from Switzerland. Health Policy. 2006 Aug;78(1):77–92.
2. Harbarth S, Monnet DL. Cultural and socioeconomic determinants of antibiotic use. In: Harbarth S, Monnet DL, editors. Antibiotic policies: fighting resistance. New York: Springer; 2008. p. 29–40. Available from: http://link.springer.com/chapter/10.1007/978-0-387-70841-6_3
3. Masiero G, Filippini M, Ferech M, Goossens H. Socioeconomic determinants of outpatient antibiotic use in Europe. Int J Public Health. 2010;55(5):469–478.
4. Klein EY, Makowsky M, Orlando M, Hatna E, Braykov NP, Laxminarayan R. Influence of provider and urgent care density across different socioeconomic strata on outpatient antibiotic prescribing in the USA. J Antimicrob Chemother. 2015 Jan;70(5):1580–7.
5. Okeke IN. Poverty and Root Causes of Resistance in Developing Countries. In: Sosa A de J, Byarugaba DK, Amábile-Cuevas CF, Hsueh P-R, Kariuki S, Okeke IN, editors. Antimicrobial Resistance in Developing Countries. New York: Springer; 2010. p. 27–35. Available from: http://link.springer.com/chapter/10.1007/978-0-387-89370-9_3
6. Gelband H, Miller-Petrie M, Pant S, Gandra S, Levinson J, Barter D, White A, Ramanan L. The State of the World’s Antibiotics, 2015. Washington DC: Center for Disease Dynamics, Economics & Policy; 2015.
7. East Africa Public Health Laboratory Networking Project. Strengthening the Role of Laboratories in Tracking Antimicrobial Drug Resistance in East Africa: Final Report to the World Bank. Washington DC: Center for Disease Dynamics, Economics & Policy; 2016.
8. European Centre for Disease Prevention and Control. Surveillance of antimicrobial consumption in Europe 2012. Stockholm: ECDC; 2014.
9. Alvarez-Uria G, Gandra S, Laxminarayan R. Poverty and prevalence of antimicrobial resistance in invasive isolates. Int J Infect Dis. 2016 Nov;52:59–61.
10. Center for Disease Dynamics, Economics & Policy. ResistanceMap. N.d. Available from: http://kinwahlin.wordpress.com/2011/09/23/resistancemap-center-for-disease-dynamics-economics-policy-us/
11. European Centre for Disease Prevention Control. Antimicrobial resistance surveillance in Europe 2015: Annual report of the European Antimicrobial Resistance Surveillance Network (EARS-Net). Stockholm: ECDC; 2017.
12. Australian Staphylococcal Sepsis Outcome Program (ASSOP) 2015 Final Report. Murdoch, Australia: The Australian Group on Antimicrobial Resistance; 2016.
13. Abdulgader SM, Shittu AO, Nicol MP, Kaba M. Molecular epidemiology of Methicillin-resistant Staphylococcus aureus in Africa: a systematic review. Front Microbiol. 2015 Apr 30;6:348. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4415431/
14. Pan American Health Organziation. Informe Anual de la Red de Monitoreo/ Vigilancia de la Resistencia a los Antibióticos y de Infecciones Asociadas a la Atención de la Salud: 2014. Unpublished.
15. Aiken AM, Karuri DM, Wanyoro AK, Macleod J. Interventional studies for preventing surgical site infections in sub-Saharan Africa – A systematic review. Int J Surg. 2012;10(5):242–9.
16. Van Boeckel TP, Gandra S, Ashok A, Caudron Q, Grenfell BT, Levin SA, Laxminarayan R. Global antibiotic consumption 2000 to 2010: An analysis of national pharmaceutical sales data. Lancet Infect Dis. 2014;14(8):742–50.
17. Van Boeckel TP, Brower C, Gilbert M, Grenfell BT, Levin SA, Robinson TP, Teillant A, Laxminarayan R. Global trends in antimicrobial use in food animals. Proc Natl Acad Sci. 2015;112(18):5649–5654.
18. Laxminarayan R, Van Boeckel TP, Teillant A. The Economic Costs of Withdrawing Antimicrobial Growth Promoters from the Livestock Sector. OECD Food, Agriculture and Fisheries Papers, No. 78. Paris: OECD Publishing; 2015.
19. Centers for Disease Prevention and Control. Antibiotic Resistance Threats in the United States, 2013. Atlanta: CDC; 2013. Available from: http://www.cdc.gov/drugresistance/threat-report-2013/
20. Pisani E. Antimicrobial resistance: What does medicine quality have to do with it? London: The Review on Antimicrobial Resistance; 2015.
21. Ocan M, Obuku EA, Bwanga F, Akena D, Richard S, Ogwal-Okeng J, Obua C. Household antimicrobial self-medication: a systematic review and meta-analysis of the burden, risk factors and outcomes in developing countries. BMC Public Health. 2015 Aug 1;15(1):742.
22. World Health Organization. Worldwide country situation analysis: response to antimicrobial resistance. Geneva: WHO; 2015.
23. Kelesidis T, Falagas ME. Substandard/counterfeit antimicrobial drugs. Clin Microbiol Rev. 2015 Apr;28(2):443–64.
24. Morgan DJ, Okeke IN, Laxminarayan R, Perencevich EN, Weisenberg S. Non-prescription antimicrobial use worldwide: a systematic review. Lancet Infect Dis. 2011 Sep;11(9):692–701.
25. Alsan M, Schoemaker L, Eggleston K, Kammili N, Kolli P, Bhattacharya J. Out-of-pocket health expenditures and antimicrobial resistance in low-income and middle-income countries: an economic analysis. Lancet Infect Dis. 2015 Oct;15(10):1203–10.
26. Alhomoud F, Aljamea Z, Almahasnah R, Alkhalifah K, Basalelah L, Alhomoud FK. Self-medication and self-prescription with antibiotics in the Middle East – do they really happen? A systemic review of the prevalence, possible reasons and outcomes. Int J Infect Dis. 2017 Apr;57:3-12. Available from: /article/S1201-9712(17)30017-6/abstract
27. Fick J, Soderstrom H, Lindberg RH, Phan C, Tysklind M, Larsson JDG. Contamination of Surface, Ground, and Drinking Water From Pharmaceutical Production. Environ Toxicol Chem. 2009;28(12):2522–7.
28. Escobar M-L, Griffin CC, Shaw RP, editors. Impact of health insurance in low- and middle-income countries. Washington, DC: The Brookings Institution; 2010.
29. Fadare JO, Adeoti AO, Aina F, Solomon OA, Ijalana JO. The influence of health insurance scheme on the drug prescribing pattern in a Nigerian tertiary healthcare facility. Niger Med J. 2015;56(5):344-8.
30. Whitehead M, Dahlgren G, Evans T. Equity and health sector reforms: can low-income countries escape the medical poverty trap? Lancet. 2001 Sept;358(9284):833-6.
31. Li S, Laxminarayan R. Are Physicians’ Prescribing Decisions Sensitive to Drug Prices? Evidence from a Free-antibiotics Program. Health Econ. 2015;24(2):158–174.
32. Matuz M, Benko R, Doro P, Hajdu E, Nagy G, Nagy E, Monnet DL, Soos G. Regional variations in community consumption of antibiotics in Hungary, 1996-2003. Br J Clin Pharmacol. 2006 Jan;61(1):96–100.
33. Md Rezal RS, Hassali MA, Alrasheedy AA, Saleem F, Md Yusof FA, Godman B. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: a systematic review of the literature. Expert Rev Anti Infect Ther. 2015 May;13(5):665–680.
34. Linder JA, Doctor JN, Friedberg MW, Reyes Nieva H, Birks C, Meeker D, Fox CR. Time of day and the decision to prescribe antibiotics. JAMA Intern Med. 2014 Dec;174(12):2029–31.
35. Teixeira Rodrigues A, Ferreira M, Piñeiro-Lamas M, Falcão A, Figueiras A, Herdeiro MT. Determinants of physician antibiotic prescribing behavior: a 3 year cohort study in Portugal. Curr Med Res Opin. 2016 May;32(5):949–57.
36. Braykov NP, Morgan DJ, Schweizer ML, Uslan DZ, Kelesidis T, Weisenberg SA, Johannsson B, Young H, Cantey J, Srinivasan A, Perencevich E, Septimus E, Laxminarayan R. Assessment of empirical antibiotic therapy optimisation in six hospitals: an observational cohort study. Lancet Infect Dis. 2014;14(12):1220–7.
37. Gerber JS, Prasad PA, Localio AR, Fiks AG, Grundmeier RW, Bell LM, Wasserman RC, Rubin DM, Keren R, Zaoutis TE. Racial differences in antibiotic prescribing by primary care pediatricians. Pediatrics. 2013 Apr;131(4):677–84.
38. Sapkota AR, Coker ME, Goldstein RER, Atkinson NL, Sweet SJ, Sopeju PO, Ojo MT, Otivhia E, Ayepola OO, Olajuyigbe OO, Shireman L, Pottinger P, Ojo KK. Self-medication with antibiotics for the treatment of menstrual symptoms in southwest Nigeria: a cross-sectional study. BMC Public Health. 2010 Oct 15;10(1):610.


