
Rosanna W Peeling (left), Professor and Chair of Diagnostics Research and Debrah I Boeras (Right), Diagnostics Consultant, International Diagnostics Centre, London School of Hygiene & Tropical Medicine, United Kingdom
Bacterial and viral infections are often clinically indistinguishable and cannot be managed appropriately without the aid of diagnostic tests. Rapid diagnostic tests (RDTs) can be used at the point of care to guide appropriate treatment and reduce the risk of antimicrobial resistance (AMR). Developing RDTs that can be used at different levels of the healthcare system for syndromes with multiple aetiologies is complex and challenging, but promising technologies are in the pipeline. Assuring the quality of tests and testing, and ensuring linkage to appropriate antibiotic use will be critical to maximizing the benefit of RDTs and reducing the risk of antimicrobial resistance.
Antimicrobial resistance (AMR) is one of the greatest public health challenges of this century with an estimated 25 000 deaths and over €1.5 billion a year in healthcare expenses and productivity losses in Europe alone. The EU/USA Transatlantic Task Force on AMR (TATFAR) and The Joint Programming Initiative on Antimicrobial Resistance (JPIAMR), signed by 22 countries, are examples of national and international efforts aimed at reducing the emerging antimicrobial resistance risks and preserving antibiotics for future generations (1, 2).
There are many national strategies to combat antimicrobial resistance and they consist of multi-pronged approaches. As an example, the United Kingdom’s antimicrobial resistance strategy aims to achieve the following by 2018 (3):
- Good infection prevention and control measures to help prevent infections occurring become the norm in all sectors of human and animal health.
- Infections can be diagnosed quickly and the right treatment used.
- Patients and animal keepers fully understand the importance of antibiotic treatment regimens and adhere to them.
- Surveillance is in place which quickly identifies new threats or changing patterns in resistance.
- There is a sustainable supply of new, effective antimicrobials.
Two of the five targets above require diagnostics that allow rapid identification of infections to reduce inappropriate antibiotic prescriptions, and assays that can be used to identify and track patterns of antimicrobial resistance. As an incentive for drug companies to develop new antimicrobials, having accurate rapid diagnostic tests (RDTs) that can be used at the point of care can reduce the cost and length of drug trials, as target populations for clinical trials could be identified and recruited without expensive laboratory tests and procedures.
Access to appropriate diagnosis and treatment remains a top priority to reduce the enormous burden of infectious diseases in the developing world (4). In countries where laboratory services are not widely available, the World Health Organization (WHO) recommends syndromic management in which patients are treated for all major causes of the syndrome. For the Integrated Management of Childhood Illness, WHO recommended that children with fever in malaria-endemic areas be presumptively treated with antimalarial drugs, unless they have a cough and a rapid respiratory rate, in which case they should also receive antibiotics. Malaria RDTs and a urine dipstick test for febrile children two years of age or older with abdominal tenderness have since been added to these guidelines. Children RDT-negative are classified as “likely viral infection.” However, a study in Tanzania showed that although the use of malaria RDTs resulted in a reduction from 75% to 20% in the proportion of patients receiving anti-malarial treatment, there was a concomitant increase in antibiotic prescription from 49% to 72% (5). The increase in antibiotic prescription is neither evidence-based nor likely effective, as a study in an outpatient clinic in Tanzania showed that 71% of children presenting with fever had viral infections, 22% had bacterial infections, and 11% had parasitic infections (6). Bacterial and viral infections are often clinically indistinguishable and cannot be managed appropriately without the aid of diagnostic tests.
Development of diagnostics to combat antimicrobial resistance
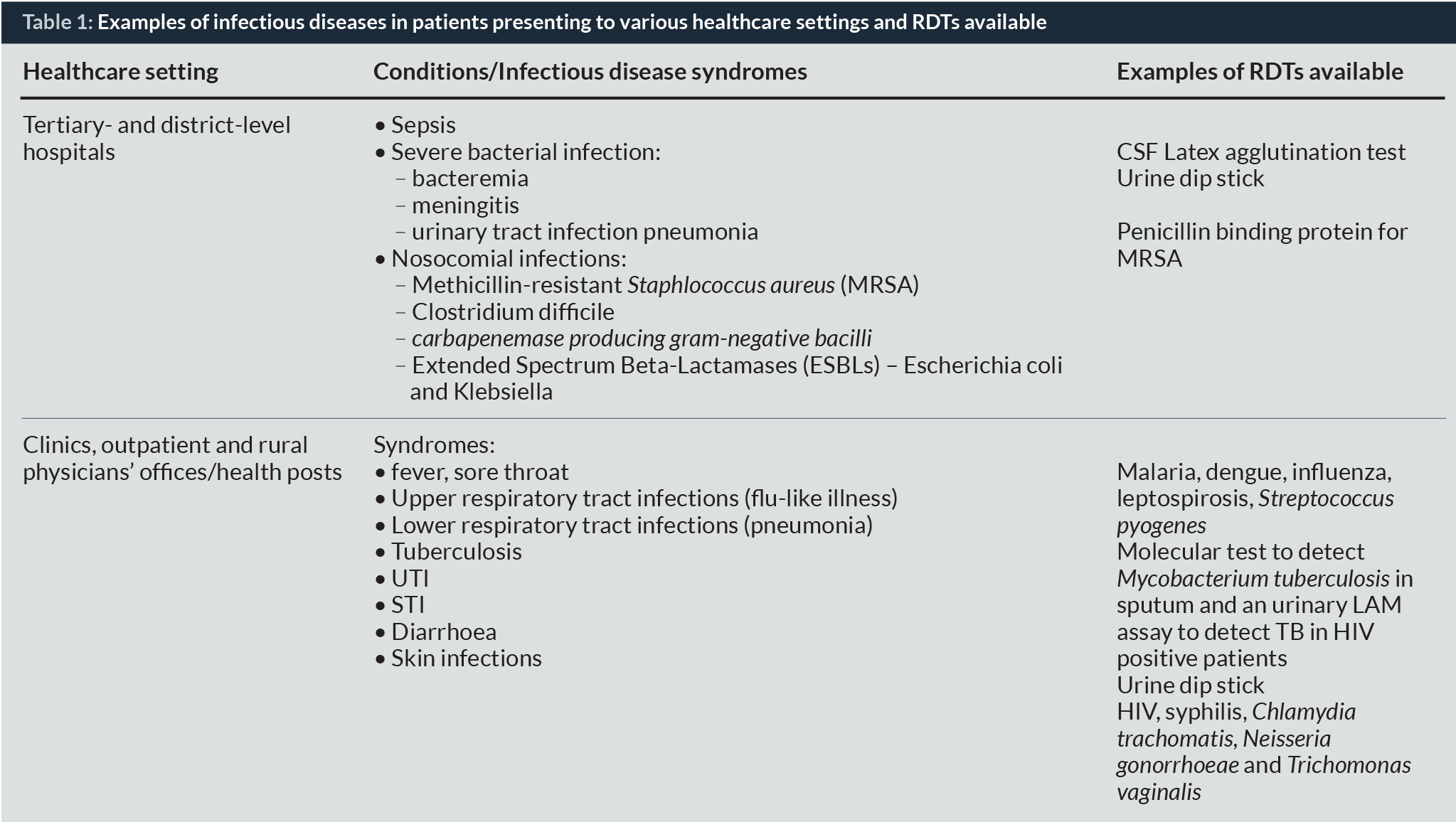
Table 1 presents examples of syndromes in patients presenting to various health settings and RDTs that are commercially available. Developing tests that can detect aetiologic agents for syndromes with multiple aetiologies present tremendous challenges for several reasons. First, the major causes of these syndromes can vary by geographic region, by rainy or dry season even within the same area, and possibly by different strains of the same pathogen. Second, capacity to perform a diagnostic test varies at different levels of the healthcare system due to human resource and environmental constraints, such as dust, humidity, heat and availability of power. WHO recommends the ASSURED benchmark for the ideal test as being Affordable, Sensitive, Specific, User-friendly in that it is easy to perform, requiring minimal training, Rapid and robust in that it can be stored at room temperature, Equipment-free or minimal equipment, and Deliverable to those who need it. It is, however, not realistic to expect that an RDT would be able to provide the same accuracy as a laboratory-based test performed by skilled technicians under optimal conditions. Test developers face the difficulty of having to make “trade-offs” between affordability, accuracy and access, depending on the level of the healthcare system at which the test will be used. Third, perhaps with the exception of tertiary care hospitals, the availability of the appropriate drugs at the point of care may be limited, even after a definitive diagnosis has been made. Severe febrile illness in the tropics could be due to malaria, pneumonia, dengue, enteric fever, leptospirosis, meningococcal infection, brucellosis, visceral leishmaniasis, relapsing fever or human African trypanosomiasis (7). These severe yet treatable infections require specific therapy, and should not be treated presumptively with antibiotics.
Diagnostic tests using host biomarkers
For syndromes with multiple aetiologies, it is unlikely that a single RDT would be available to detect all the causes of the syndrome. For patients with severe infections in hospital settings, timely diagnosis and treatment is critical, but identifying specific pathogens may take time. Studies have been conducted to determine if host biomarkers or host-proteome signatures can be used to distinguish between bacterial and viral infections.
These markers include the use of white blood count (WBC), neutrophil count, C-reactive protein (CRP), and procalcitonin to distinguish between bacterial and viral infections (8). A model based on CRP and Chitinase 3-like-1 discriminated between end-point pneumonia and non-end-point pneumonia with 93.3% sensitivity (95% confidence interval 76.5–98.8), 80.8% specificity (72.6–87.1), and a misclassification rate 0.20 (standard error 0.038) (9). In a study of CRP concentration, WBC, and absolute neutrophil count in patients with severe bacterial infection (SBI), only CRP remained as a predictor of SBI (10). A CRP cut-off point of 7 maximized both sensitivity and specificity (sensitivity 79%, specificity 91%, likelihood ratio 8.3, 95% CI: 3.8, 27.3) while a CRP concentration of <5 mg/dL effectively ruled out SBI (likelihood ratio 0.087, 95% CI: 0.02, 0.38). A study of host biomarkers showed that a host-proteome signature compromising CRP, TNF Related Apotosis Inducing Ligand (TRAIL) and Interferon-gamma inducible Protein-10 (IP-10) are most useful for distinguishing between bacterial and viral infections (11).
Development of novel diagnostics
Although host proteome signature may allow distinction between bacterial and viral infections and reduce antibiotic use, it is not sufficient to guide appropriate antibiotic use. Promising high throughput array technologies for pathogen detection, coupled with detection of antimicrobial susceptibility patterns for AMR, surveillance will be needed to guide patient management and improve our understanding of the emergence and spread of resistance. In recent years, developers have benefited from major investments in rapid detection technology for global security and for high profile diseases such as HIV and tuberculosis. A range of molecular assays that are highly sensitive and specific and can be performed at the point of care are now available. As these tests are in a “sample-in answer-out” format, requiring minimal training, they can be used in resource-limited settings (12). Diagnostic technologies for antimicrobial resistance currently available and in the pipeline are described in a compendium prepared by the Oxford Centre for Evidence-based Medicine (13).
Incentivizing diagnostic test development
A number of initiatives to incentivize the public and private sectors to develop RDTs and tests for antimicrobial resistance surveillance have been announced. The Longitude Prize aims to combat antimicrobial resistance with a £10 million prize fund for a diagnostic tool that can rule out antibiotic use or help identify an effective antibiotic to treat a patient. The challenge is to create a cost-effective, accurate, rapid, and easy-to-use test for bacterial infections that will allow health professionals worldwide to administer the right antibiotics at the right time. The European Commission has a Horizon 2020 prize of 1 million euros for better use of antibiotics through the development of a rapid test that will allow healthcare providers to distinguish, at the point of care, between patients with respiratory tract infections that require antibiotics and those who can be managed safely without antibiotics. The US National Institutes of Health is offering a prize of up to US$ 20 million to the first group(s) to develop a rapid, point of care diagnostic test to be used by healthcare providers to identify highly resistant bacterial infections to promote responsible use of antibiotics.
Challenges of implementing testing beyond the laboratory
While RDTs can offer rapid identification of the causes of infections and enable appropriate prescribing, taking testing outside of laboratories can add stresses to a weak or fragile healthcare system. Leadership and infrastructure for critical decision-making on the adoption of new diagnostic technologies are often fragmented or absent in many countries. Companies with novel diagnostic technologies often face long delays in regulatory approval and unnecessary expenditure associated with excessive duplication of clinical trials in countries they intend to market to. Unlike the regulation and adoption of new drugs and vaccines, global governance and oversight to ensure quality and efficiency are lacking in diagnostics.
The barriers faced in implementing testing at the point of care are often not technological, but constraints inherent in the healthcare system. To implement a successful RDT programme, the engagement of policymakers, stakeholders and partners to ensure buy-in and align necessary resources are a critical first step. Clear policy to guide RDT use and informed decisions are needed on strategic placement of RDTs where appropriate antibiotics are available. Training of vast numbers of healthcare providers to use RDTs, and ensuring an effective supply chain for tests and drugs across the country present an enormous challenge to health systems that are already suffering from a critical shortage of human resources. Quality assurance systems are essential to ensure accurate results are being used to guide treatment decisions, and to ensure that antimicrobial resistance control strategies are based on accurate surveillance data. Technical support is needed to support every point of testing. Costs and cost-effectiveness. Studies have shown that deployment of RDTs can be an opportunity to improve health outcomes and strengthen healthcare systems (15, 16). Overcoming challenges will in turn motivate healthcare workers and increase capacity and efficiency to test and treat appropriately. RDT introduction and implementation must be culturally sensitive and accompanied by an interconnected system to monitor the necessary processes.
Need for connectivity
In 2001, Heymann and Rodier drew our attention to the capability of “infectious disease intelligence” to improve early warning capacity for potential worldwide public health problems and possibly diminish or even prevent the spread of infectious diseases (17). Connectivity solutions for testing at the point of care can now be used to provide timely information on testing, trends and quality assurance, and can be coupled to optimize supply chain management (18, 19). Alerts can be built into connectivity systems to support disease surveillance and outbreak investigations.
Tests for antimicrobial resistance surveillance
Monitoring and identifying imported infections and carriage of organisms with antimicrobial resistance is critical for plans of action. The Global Antimicrobial Resistance Surveillance System (GLASS) aims to standardize the collection, analysis and sharing of data on AMR to provide the evidence base for action. The European Antimicrobial Resistance Surveillance Network (EARS-Net) is a coordinated surveillance network sharing data on the occurrence and spread of AMR in European countries through an interactive database. EARS-Net provides trends and country and geographical overviews of antimicrobial consumption as well as quality indicators. A recent report from Ghana shows the importance of antimicrobial resistance surveillance to ensure that antibiotics recommended in national guidelines are still effective.
Conclusion
RDTs can be used to guide appropriate treatment at the point of care and reduce the risk of antimicrobial resistance. Substantial research effort is urgently needed to accelerate the development, validation and deployment of RDTs that can aid clinical management decisions in patients presenting with major syndromes for which antibiotics are currently prescribed, but which may be of viral origin. Combining pathogen detection with host proteomic signatures holds promise for distinguishing between bacterial and viral infections. High throughput molecular tests for identifying susceptibility patterns as part of AMR surveillance will improve our understanding of factors that can reduce the risk of emergence and spread of antimicrobial resistance. While decentralization of testing for infectious diseases can impose enormous stress on weak or fragile health systems, improving access to evidence-based management of patients provides an opportunity to make health systems more efficient and improve patient outcomes. Quality assurance and linkage to appropriate treatment and care will be critical to maximizing the benefit of RDTs. Surveillance systems with connectivity at national, regional and global levels are important to monitor antimicrobial resistance trends, and identify interventions with significant impacts on reducing the risk of antimicrobial resistance.
Biographies
Dr Debrah Boeras is a diagnostics consultant working with the London School of Hygiene and Tropical Medicine’s International Diagnostic Centre to improve access to diagnostics and quality of testing in resource-limited settings. She previously worked at the International Laboratory Branch at the US Centers for Disease Control and Prevention to strengthen molecular diagnostics in collaboration with Ministries of Health and international agencies to ensure the introduction of accessible quality diagnostics will impact patient care.
To download a PDF of this article click here
“We hope that you will enjoy the 2016 edition of AMR Control.”
References
1. Centers for Disease Control and Prevention. Transatlantic Task Force on Antimicrobial Resistance (TATFAR) 2009. Available from: http://www.cdc.gov/drugresistance/tatfar/.
2. Joint Programming Initiative on Antimicrobial Resistance. The Joint Programming Initiative on Antimicrobial Resistance. 2015.
3. Department of Health. UK 5 Year Antimicrobial Resistance Strategy 2013 to 2018.
4. Feikin DR, Olack B, Bigogo GM, Audi A, Cosmas L, Aura B, et al. The burden of common infectious disease syndromes at the clinic and household level from population-based surveillance in rural and urban Kenya. PLoS One. 2011;6(1):e16085.
5. D’Acremont V, Kahama-Maro J, Swai N, Mtasiwa D, Genton B, Lengeler C. Reduction of anti-malarial consumption after rapid diagnostic tests implementation in Dar es Salaam: A before-after and cluster randomized controlled study. Malar J. 2011;10:107.
6. D’Acremont V, Kaiser L, Genton B. Causes of fever in outpatient Tanzanian children. N Engl J Med. 2014;370(23):2243-4.
7. Chappuis F, Alirol E, d’Acremont V, Bottieau E, Yansouni CP. Rapid diagnostic tests for non-malarial febrile illness in the tropics. Clin Microbiol Infect. 2013;19(5):422-31.
8. Lubell Y, Blacksell SD, Dunachie S, Tanganuchitcharnchai A, Althaus T, Watthanaworawit W, et al. Performance of C-reactive protein and procalcitonin to distinguish viral from bacterial and malarial causes of fever in Southeast Asia. BMC Infect Dis. 2015;15:511.
9. Erdman LK, D’Acremont V, Hayford K, Rajwans N, Kilowoko M, Kyungu E, et al. Biomarkers of Host Response Predict Primary End-Point Radiological Pneumonia in Tanzanian Children with Clinical Pneumonia: A Prospective Cohort Study. PLoS One. 2015;10(9):e0137592.
10. Pulliam PN, Attia MW, Cronan KM. C-reactive protein in febrile children 1 to 36 months of age with clinically undetectable serious bacterial infection. Pediatrics. 2001;108(6):1275-9.
11. Oved K, Cohen A, Boico O, Navon R, Friedman T, Etshtein L, et al. A novel host-proteome signature for distinguishing between acute bacterial and viral infections. PLoS One. 2015;10(3):e0120012.
12. Peeling RW, McNerney R. Emerging technologies in point-of-care molecular diagnostics for resource-limited settings. Expert Rev Mol Diagn. 2014;14(5):525-34.
13. University of Oxford. Centre for Evidence-based Medicine 2015. Available from: http://www.cebm.net/diagnostic-technologies-for-antimicrobial-resistance/.
14. Okeke IN, Peeling RW, Goossens H, Auckenthaler R, Olmsted SS, de Lavison JF, et al. Diagnostics as essential tools for containing antibacterial resistance. Drug Resist Updat. 2011;14(2):95-106.
15. Mabey DC, Sollis KA, Kelly HA, Benzaken AS, Bitarakwate E, Changalucha J, et al. Point-of-care tests to strengthen health systems and save newborn lives: The case of syphilis. PLoS Med. 2012;9(6):e1001233.
16. Garcia PJ, Carcamo CP, Chiappe M, Valderrama M, La Rosa S, Holmes KK, et al. Rapid Syphilis Tests as Catalysts for Health Systems Strengthening: A Case Study from Peru. PLoS One. 2013;8(6):e66905.
17. Heymann DL, Rodier GR, WHO Operational Support Team to the Global Outbreak Alert and Response Network. Hot spots in a wired world: WHO surveillance of emerging and re-emerging infectious diseases. Lancet Infect Dis. 2001;1(5):345-53.
18. Wedderburn CJ, Murtagh M, Toskin I, Peeling RW. Using electronic readers to monitor progress toward elimination of mother-to-child transmission of HIV and syphilis: An opinion piece. Int J Gynaecol Obstet. 2015;130 Suppl 1:S81-3.
19. Peeling RW. Diagnostics in a digital age: an opportunity to strengthen health systems and improve health outcomes. Int Health. 2015;7(6):384-9.
20. Opintan JA, Newman MJ, Arhin, RE, Donkor ES, Gyansa-Lutterodt M, Mills-Pappoe W. Laboratory-based nationwide surveillance of antimicrobial resistance in Ghana. Infection and Drug Resistance 2015:8 379–389.